Cardiac myocytes are the most physically energetic cells in the body. They are highly specialized high-oxygen-content cells that house a large number of mitochondria. They occupy as much as 75% of the cardiac mass, but constitute only about one third of the total cell number in the heart. Differentiated cardiac myocytes have little capacity to proliferate; however, hypertrophic growth has been shown to respond to alpha1-adrenergic stimuli via the Ras/MEK pathway. All cardiac myocytes are capable of spontaneous rhythmic depolarization and repolarization of their membranes. Contraction of cardiac myocytes is myogenic, which is independent of nervous stimulation. There is a complex network of signals in cardiac myocytes regulating the rhythmic pumping of the heart. Cardiac myocyte hypertrophy and apoptosis have been implicated in the loss of contractile function during heart failure. A better understanding of the cardiac signaling network will help reveal the cellular mechanisms leading to cardiac myocyte death.
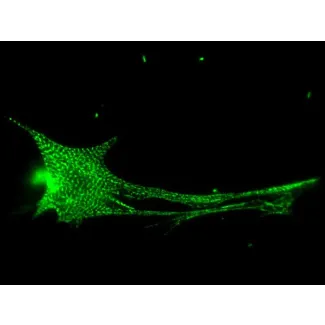
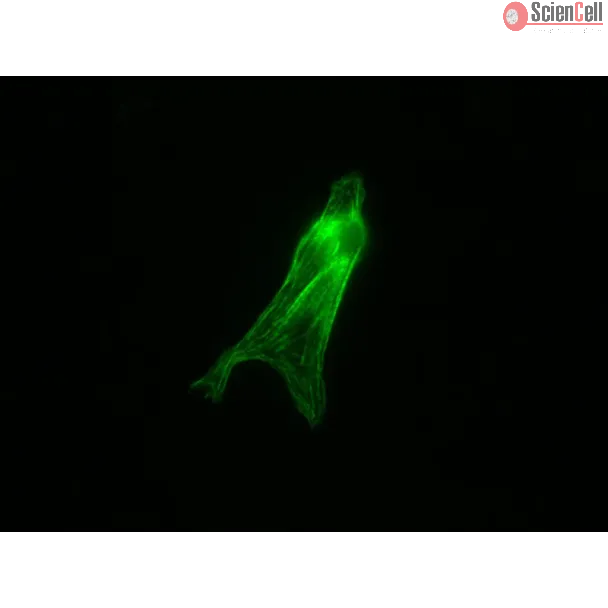
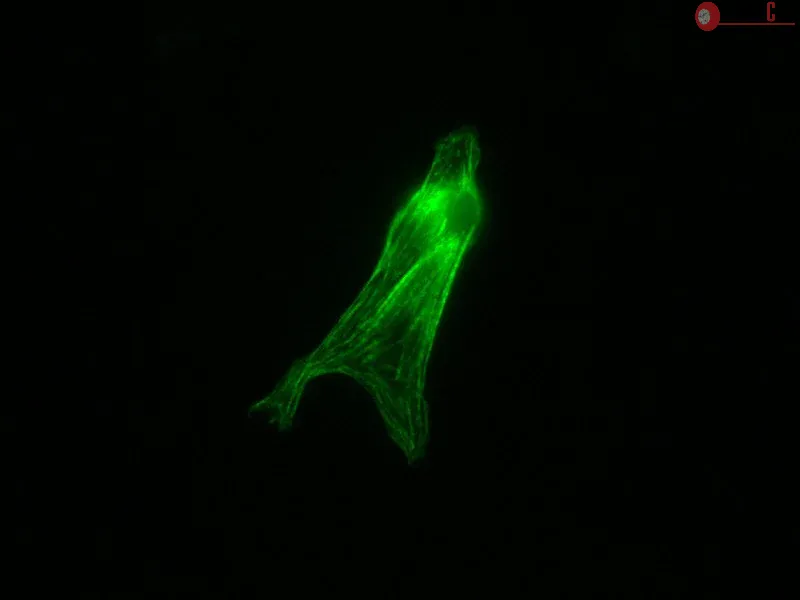
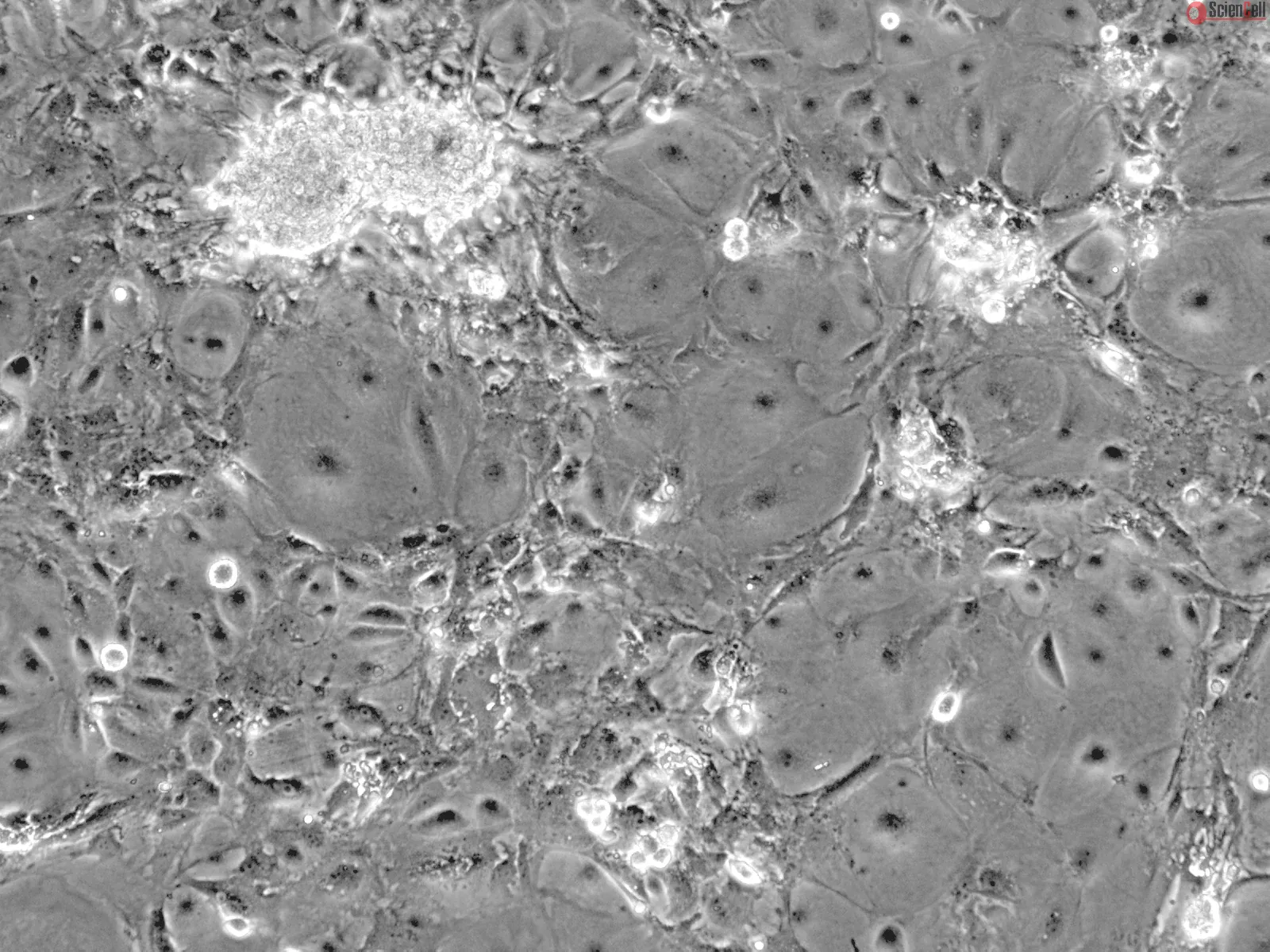
Mouse Cardiac Myocytes from CD1 (MCM) ScienCell Research Laboratories are isolated from postnatal day 2 or postnatal day 8 CD-1 mouse heart. MCM are cryopreserved at P0 and delivered frozen. Each vial contains >1 x 106 cells in 1 ml volume. MCM are characterized by immunofluorescence with antibodies specific to sarcomeric alpha-actinin and/or α-smooth muscle actin. MCM are negative for mycoplasma, bacteria, yeast, and fungi. MCM are guaranteed to further culture under the conditions provided by ScienCell Research Laboratories; however, MCM are not recommended for expanding or long-term cultures since the cells do not proliferate in culture.
Recommended Medium
It is recommended to use Cardiac Myocyte Medium-serum free (CMM-sf, Cat. #6101) for culturing MCM in vitro.
The clinical controversy of rosiglitazone as a hypoglycemic agent is potentially associated with heart failure, mainly due to its potent activation of peroxisome prolifer... More
The clinical controversy of rosiglitazone as a hypoglycemic agent is potentially associated with heart failure, mainly due to its potent activation of peroxisome proliferator-activated receptor γ (PPARγ). PPARγ partial agonists showed superior pharmacological profiles to rosiglitazone. This study compared differences in cardiac morphology and function of the PPARγ partial agonist CMHX008 with rosiglitazone. High-fat diet (HFD) induced obese mice, ob/ob mice and cardiomyocytes overexpressing PPARγ2 were treated with CMHX008 or rosiglitazone. Heart function, myocardial morphology, and hypertrophy-related gene expression were examined. Clinical information from patients with type 2 diabetes mellitus (T2DM) who had taken rosiglitazone and undergone Doppler echocardiography was collected. HFD and ob/ob mice significantly developed cardiac contractile dysfunction, with upregulated PPARγ2 protein levels in heart tissues. Cardiomyocytes of HFD and ob/ob mice were disorderly arranged, the cell areas expanded, and collagen accumulated. In vitro cardiomyocytes overexpressing PPARγ2 displayed obvious structural abnormalities and high mRNA levels of ANP and BNP, critical cardiac hypertrophy-related genes. HFD-fed mice treated with rosiglitazone or CMHX008 had significantly improved cardiac function, but rosiglitazone induced higher expression of ANP and βMHC and hypertrophic cardiomyopathy, while CMHX008 did not. Patients with T2DM taking rosiglitazone exhibited increased thickness of the posterior wall and the ventricular septum, suggesting cardiac hypertrophy. Our findings show that diabetic cardiomyopathy was associated with ectopic overexpression of PPARγ2. The full agonist rosiglitazone prevents cardiac dysfunction at the expense of compensatory hypertrophy, while the partial agonist CMHX008 shared a comparable protective effect without altering the structure of cardiomyocytes. Less
Myocardial ischemia/reperfusion (I/R) injury may cause the apoptosis of cardiomyocytes as well as cardiac fibrosis, which is characterized as the transdifferentiation of ... More
Myocardial ischemia/reperfusion (I/R) injury may cause the apoptosis of cardiomyocytes as well as cardiac fibrosis, which is characterized as the transdifferentiation of fibroblasts to myofibroblasts and collagen deposition. MicroRNAs (miRNAs or miRs) have been demonstrated to be involved in myocardial I/R injury. However, the underlying molecular mechanism remains largely unclear. In the present study, mouse cardiomyocyte M6200 cells were treated with hypoxia/reoxygenation (H/R). Our data indicated that H/R treatment led to cell apoptosis, the increased expression of fibrosis‑related proteins, namely collagen I, II, III, and fibronectin, as well as the downregulation of miR-142-3p in M6200 cells. Overexpression of miR-142-3p suppressed the H/R-induced apoptosis and fibrosis of M6200 cells. Bioinformatics analysis and a Dual‑Luciferase reporter assay further identified high mobility group box 1 (HMGB1) as a direct target gene of miR-142-3p, and miR-142-3p negatively regulated the protein level of HMGB1 in M6200 cells. Furthermore, knockdown of HMGB1 enhanced cell proliferation whereas it inhibited the apoptosis and fibrosis of M6200 cells. In addition, TGF-β1/Smad3 signaling was suggested to be involved in the miR-142-3p/HMGB1-mediated apoptosis and fibrosis of M6200 cells treated with H/R. Taken together, the findings of the present study demonstrate that miR-142-3p inhibits H/R-induced apoptosis and fibrosis of cardiomyocytes, partly at least, by the direct inhibition of HMGB1 expression. Therefore, these findings have increased our understanding of the pathogenesis of H/R-induced myocardial injury. Less
ScienCell Research Laboratories (SRL) takes pride in being a resource for researchers all over the world. The publications listed here are not meant as an endorsement or confirmation of the reliability of the products.

,-1-mg-ml--2.jpg)